Ultrasound Case: Umbilical Endometriosis
Clinical History
A 34-year-old nulliparous female presented to the imaging department with a 6-month history of a painful, swelling umbilical nodule. The patient reported that the pain was distinctly cyclical, exacerbating sharply just before and during her menstrual period. Over the last three cycles, she noted spontaneous dark-brown bleeding and discharge from the umbilicus during her menses. She had no prior history of abdominal or pelvic surgeries (e.g., laparoscopy) and no formal diagnosis of pelvic endometriosis, though she noted a history of moderate dysmenorrhea. On physical examination, a firm, bluish-purple, tender nodule measuring approximately 1.5cm was palpated within the umbilical cleft.
Ultrasound Findings
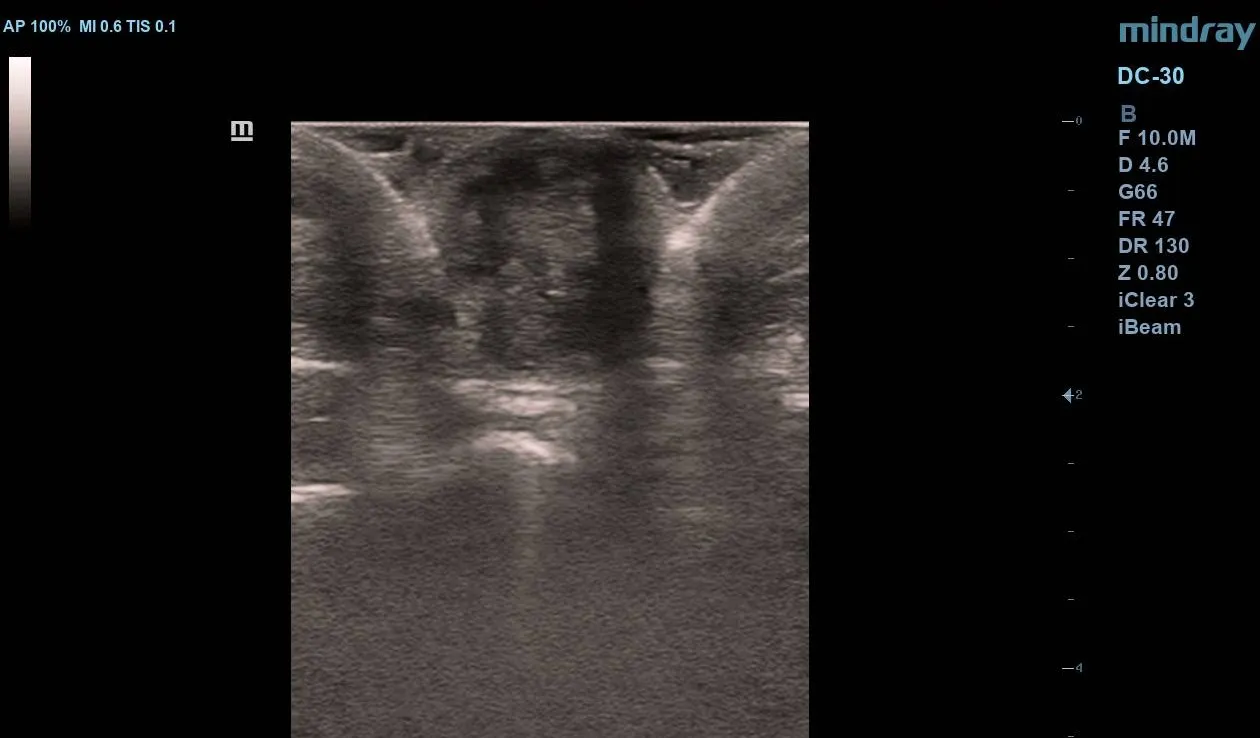
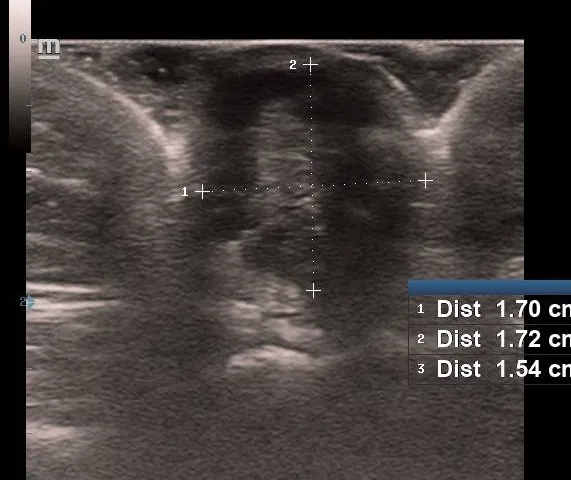
Transcutaneous ultrasound of the umbilicus using a high-frequency linear transducer revealed:
- A well-defined, mildly irregular, hypoechoic solid nodule measuring (1.72 x 1.54 x 1.70)cm within the subcutaneous tissue of the umbilicus.
- Internal tiny echogenic foci, highly suggestive of small endometrial glands.
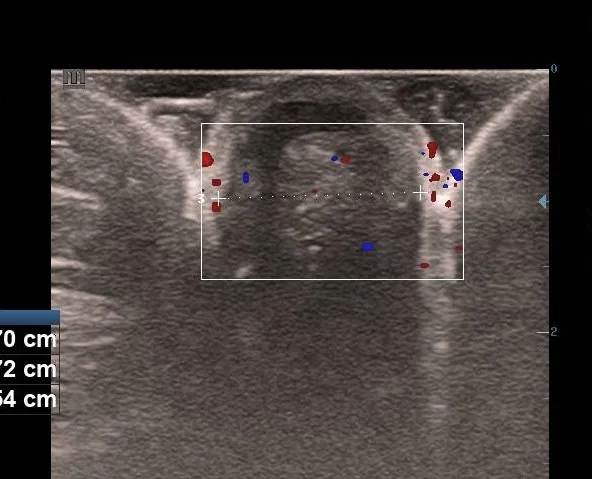
- Color Doppler application demonstrates mild internal and peripheral vascularity, showing a low-resistance flow pattern. Importantly, there was no deep extension into the rectus fascia or peritoneum.
Management and Histopathology
Given the symptoms and definitive imaging, a provisional diagnosis of umbilical endometriosis was made. The patient underwent a wide local excision of the umbilical mass with preservation of the umbilical ring, under general anesthesia. Histopathological examination confirmed the diagnosis, revealing:
- Endometrial glands lined by pseudostratified columnar epithelium.
- Surrounding cellular endometrial stroma.
- Extensive extracellular hemosiderin deposits and chronic inflammatory infiltrates, validating the cyclic bleeding reported by the patient.
Differential Diagnosis
The clinical triad of an umbilical mass, cyclical pain, and bleeding is highly pathognomonic. However, because practitioners often fail to connect umbilical symptoms with the menstrual cycle, misdiagnoses are common. The differential diagnosis includes:
- Sister Mary Joseph Nodule: Metastatic adenocarcinoma (usually gastric, ovarian, or colorectal), which typically presents as a hard, non-cyclical, ulcerated nodule.
- Pyogenic Granuloma: Vascular or pigmented cutaneous lesions.
- Umbilical Hernia: Usually reducible, cough-impulse positive, and lacks cyclical changes.