Ultrasound Case: Pleomorphic Adenoma of the Parotid Gland
Clinical History
A 44-year-old male patient presented with a painless swelling in the right pre-auricular region, progressively increasing in size over several months. There was no history of pain, facial nerve weakness, skin ulceration, or systemic symptoms. On physical examination, the swelling was located in the right pre-auricular area (anatomically corresponding to the parotid gland region), firm, well-defined, non-tender, and mobile over underlying structures.
Ultrasound Findings
Ultrasound examination of the parotid region demonstrated:
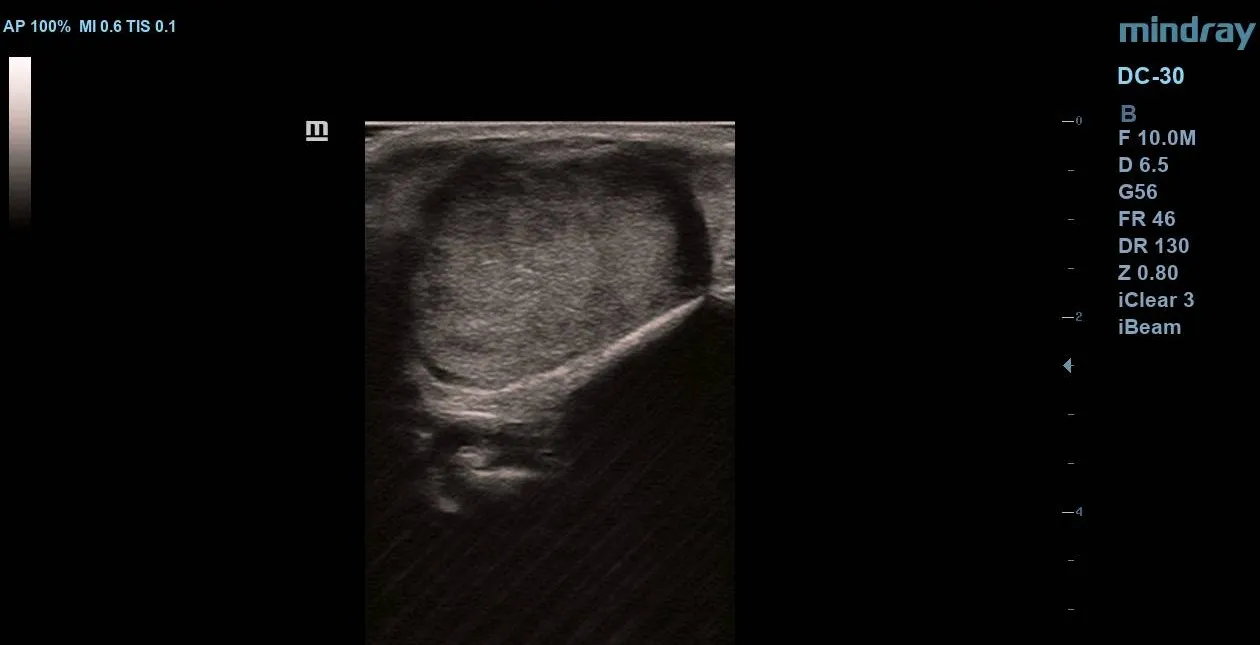
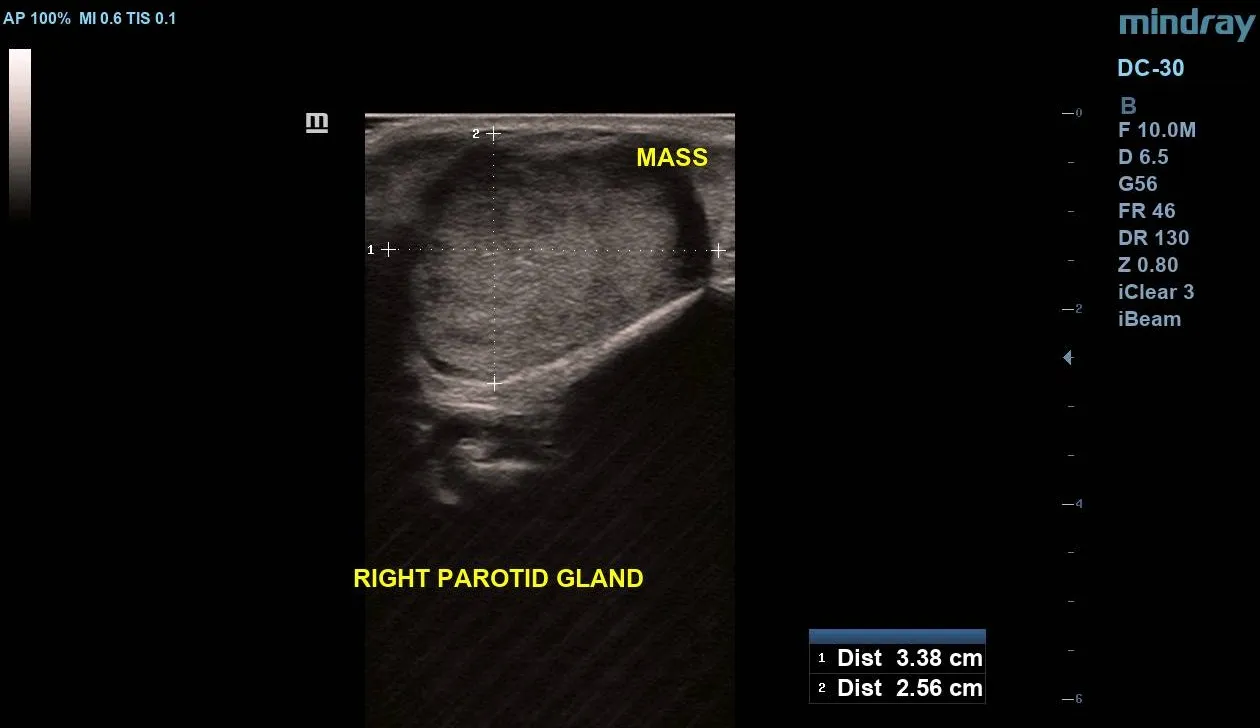
- A well-circumscribed hypoechoic solid mass within the right parotid gland.
- Measuring approximately 3.38 cm × 2.56 cm.
- Smooth margins and relatively homogeneous internal echotexture.
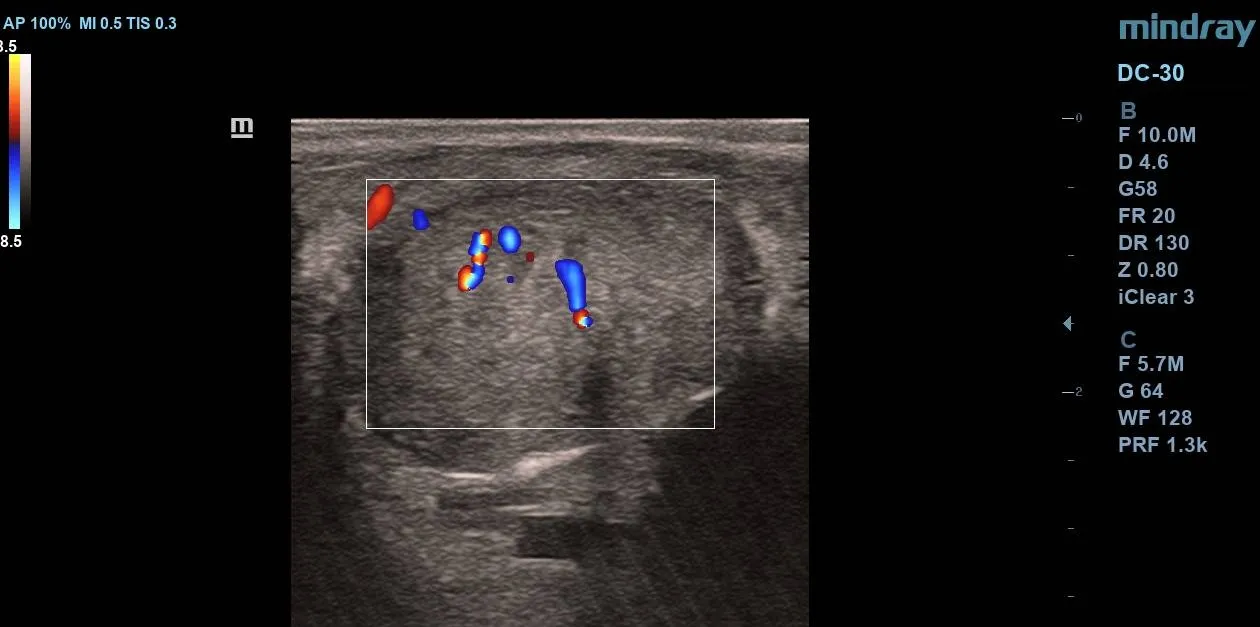
- Internal vascularity visible on colour Doppler imaging.
- No areas of cystic degeneration or calcifications were present.
- No evidence of local invasion into adjacent structures was seen.
- The contralateral parotid gland appeared normal, and no significant cervical lymphadenopathy was identified.
Diagnosis
The clinical presentation and imaging findings are highly suggestive of a pleomorphic adenoma of the right parotid gland, presenting clinically as a pre-auricular swelling. Histopathological confirmation via fine needle aspiration cytology (FNAC) or biopsy was recommended.
Discussion
Pleomorphic adenoma, also known as a benign mixed tumor, is the most common tumor of the salivary glands, most frequently arising within the superficial lobe of the parotid gland. These tumors typically contain a mixture of epithelial, myoepithelial, and stromal (mucoid, myxoid, or chondroid) components. Characteristically, they grow slowly and present as painless, firm, mobile masses.
High-resolution ultrasound is invaluable for initial assessment, characteristically demonstrating a well-defined, hypoechoic or lobulated mass with posterior acoustic enhancement (even though solid) and varying degrees of internal vascularity. While predominantly benign, accurate characterization is essential to differentiate them from malignant processes and to map their relationship with adjacent anatomical landmarks.
Differential Diagnosis
Given the pre-auricular location and solid sonographic features, key differentials include:
- Warthin Tumor (Cystadenolymphoma): The second most common benign parotid tumor, frequently found in older male patients, often bilateral or multifocal, and more prone to cystic components.
- Mucoepidermoid Carcinoma or Adenoid Cystic Carcinoma: Primary salivary malignancies that may present with irregular margins, aggressive localized acoustic shadows, local invasion, or clinical signs like facial nerve palsy and pain.
- Parotid Lymphadenopathy: Intraparotid lymph nodes showing a distinct echogenic fatty hilum, usually reactive or metastatic rather than a primary parenchymal mass.
Management
The established management plan for this patient includes:
- Surgical Excision: Definitive treatment is complete surgical removal, typically via a superficial parotidectomy or partial superficial parotidectomy.
- Facial Nerve Preservation: Meticulous dissection and preservation of the facial nerve are critical during surgery due to its close anatomical relationship running directly through the parotid gland.
- Prognosis and Follow-Up: The long-term prognosis is excellent following complete resection. However, long-term follow-up is essential because recurrence may occur if the tumor capsule is intraoperatively disrupted or incomplete margins are left.
Technical Spotlight: Mindray DC-30 Full HD
The clinical images featured in this case study were captured using the Mindray DC-30 Full HD Ultrasound System.
As demonstrated in this case, the DC-30 delivers exceptional clarity and performance for superficial and small-parts scanning, making it a reliable workhorse for everyday diagnostic imaging.
- Full HD Clarity: High-resolution imaging that brings out subtle structural details, crucial for evaluating complex fluid collections, debris, and tissue margins.
- Advanced Color Doppler: Sensitive blood flow detection to easily assess peripheral hyperemia and tissue vascularity.
- Optimized Workflow: Designed with an intuitive interface to reduce scan time and improve diagnostic throughput.
🛒 Looking to upgrade your clinic’s imaging tools? View full technical specifications, check regional pricing, and purchase the unit directly from our store:
👉 Buy the Mindray DC-30 Full HD here