Ultrasound Case: Cervical Incompetence at 18 Weeks’ Gestation
Clinical History
A patient presented to the antenatal clinic at 18 weeks’ gestation with complaints of persistent watery vaginal discharge over several hours. She denied experiencing vaginal bleeding, fever, or painful uterine contractions. There was no prior history of abdominal trauma or recent coitus. Her previous obstetric history was significant for one second-trimester miscarriage.
On physical examination:
- Abdomen: Soft, non-tender with no signs of active uterine irritability.
- Speculum examination: Pooling of clear fluid observed in the vaginal vault, highly suggestive of ruptured membranes.
- Infectious signs: No clinical signs of acute infection or active hemorrhage.
Ultrasound Findings
1. Technique
A transabdominal scan was initially performed for an overall assessment of fetal well-being, followed immediately by a transvaginal ultrasound (TVS) to achieve a high-resolution, precise evaluation of the cervical length and internal os.
2. Sonographic Findings
- Cervical Length: Markedly shortened, measuring approximately 14 mm (normal length during the second trimester is typically >25 mm).
- Internal Os: Dilated with clear evidence of membrane herniation and funneling.
- Funneling Configuration: Demonstrated a classic “U-shaped” configuration extending deeply into the cervical canal.
- Amniotic Membranes: Bulging and prolapsing directly into the endocervical canal, creating a classic “hourglass” appearance.
- Amniotic Fluid Volume: Remained within the normal range for gestational age at the immediate time of examination, despite the clinical history of leaking.
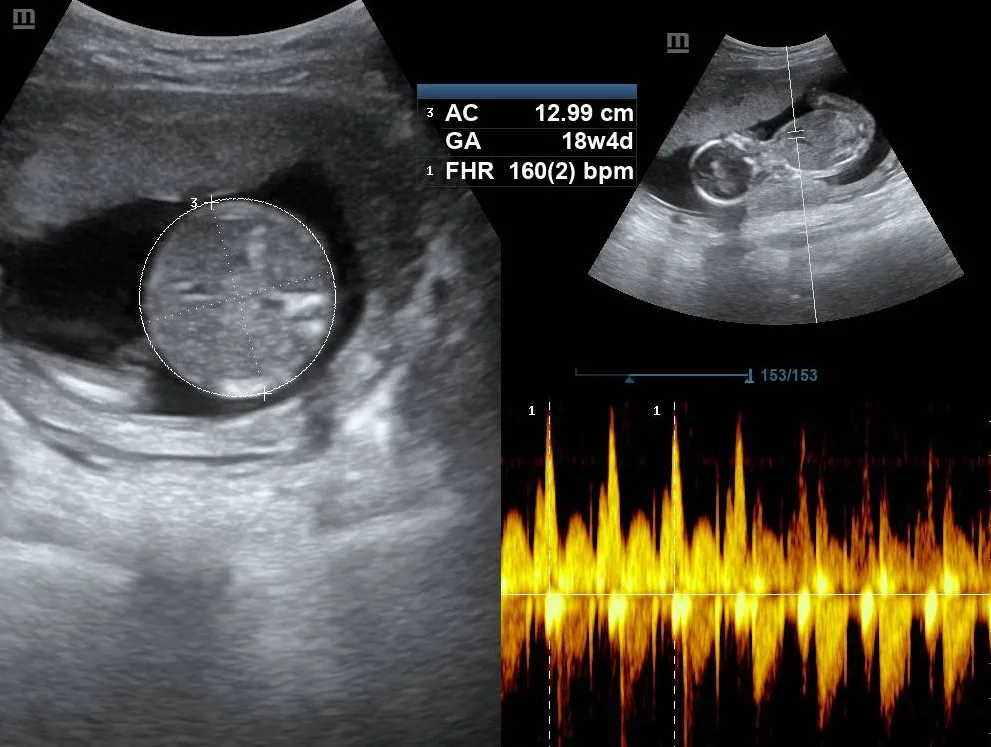
3. Fetal Status
- Viability: Single live intrauterine fetus showing dynamic, changing positions.
- Cardiac Activity: Normal cardiac activity present with a fetal heart rate (HR) of 160 bpm.
- Biometry: Normal fetal abdomen with an abdominal circumference (AC) corresponding to 18 weeks 4 days.


Conclusion
The sonographic and clinical presentation are highly consistent with cervical incompetence complicated by preterm premature rupture of membranes (PPROM). The constellation of a significantly shortened cervix (14 mm), internal os dilation, and advanced membrane prolapse provides definitive diagnostic evidence.
Discussion
Cervical incompetence (also referred to as cervical insufficiency) is a significant cause of second-trimester pregnancy loss and spontaneous preterm birth. It is clinically characterized by painless cervical shortening and dilation in the absence of uterine contractions, frequently resulting in premature rupture of membranes or inadvertent pregnancy loss.
Transvaginal sonography (TVS) stands as the gold standard imaging modality for evaluating cervical structural integrity. Key sonographic markers include a cervical length below 25 mm, dynamic cervical shortening during transfundal pressure, and progressive configurations of internal os funneling (typically transitioning from T, Y, V, to U-shaped patterns). The dynamic presentation of an advanced “U-shape” or an “hourglass” membrane prolapse carries an extremely high risk of imminent delivery.
In this index case, the structural insufficiency is unfortunately already complicated by clinical preterm premature rupture of membranes (PPROM), complicating standard management paths due to the heightened risk of ascending chorioamnionitis.