Ultrasound Case: Acute Splenic Sequestration
An 8-year-old male with HbSS disease presents with left upper quadrant pain.
Case Presentation
History
- Chief Complaint: Left upper quadrant pain and fatigue x 2 days.
- History of Present Illness: * 2-day history of worsening abdominal pain.
- Pale appearance noted by parents.
- No history of fever or trauma.
- Last blood transfusion was 6 weeks ago.
Physical Examination
- Abdomen: Tender splenomegaly (palpable 3cm below the costal margin).
- General: Pale conjunctivae.
- Lab Results: Hemoglobin: 5.2 g/dL (patient’s documented baseline is 8.0 g/dL).
Clinical Suspicion: Given the acute drop in hemoglobin accompanied by painful splenomegaly in a pediatric sickle cell patient, an acute splenic sequestration crisis is highly suspected. Emergency ultrasound is indicated to confirm splenic changes and assess for complications.
Ultrasound Findings
- Markedly enlarged spleen: Severe splenomegaly extending deep into the abdomen.
- Heterogeneous echotexture: Parenchyma displays patchy, ill-defined hypoechoic regions representing congested blood pooling.
- Decreased parenchymal flow: Doppler imaging demonstrates reduced or altered vascularity/outflow within the affected splenic tissue.
- Perisplenic fluid: A small anechoic fluid rim is visualized surrounding the spleen, indicative of trace reactive fluid.
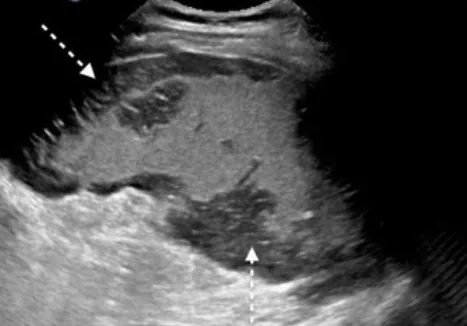
1. Splenic Sequestration: Markedly enlarged spleen demonstrating a heterogeneous parenchymal echotexture with patchy, ill-defined hypoechoic areas.

2. Perisplenic fluid: Small, localized anechoic fluid rim surrounding the outer boundary of the spleen.
Final Diagnosis: Acute Splenic Sequestration Crisis > Confirmed based on classic clinical signs (sudden, painful splenic enlargement and profound acute anemia presenting as pallor and fatigue) alongside diagnostic ultrasound features (marked splenomegaly, parenchymal heterogeneity, and decreased vascular flow properties).
Differential Diagnosis
- Splenic Infarction: Typically presents with classic wedge-shaped, well-demarcated hypoechoic lesions on ultrasound without causing significant, global organ enlargement.
- Splenic Abscess: Features complex hypoechoic or anechoic mass-like lesions containing internal debris, moving echoes, or gas-fluid levels; clinically distinguished by high spiking fevers and leukocytosis.
- Splenic Rupture: Visualized on ultrasound with irregular, disrupted splenic margins and free fluid/hemoperitoneum (often in Morison’s pouch and the pelvis); typically associated with a clear history of trauma or direct impact.