Ultrasound Case: Acute Appendicitis
A 12-year-old male presents with right lower quadrant pain and fever.
Case Presentation
History
- Chief Complaint: Right lower quadrant (RLQ) pain and fever.
- History of Present Illness:
- Periumbilical pain migrating to the RLQ over the course of 24 hours.
- Pain worsens noticeably with body movement and coughing.
- Low-grade fever (38.1°C).
- Anorexia (loss of appetite) for the past 12 hours.
- No history of diarrhea or accompanying urinary symptoms.
- Past Medical History: No previous abdominal surgeries; no similar painful episodes in the past.
- Initial Labs: WBC 14.5 × 10³/µL (neutrophil predominance), CRP 32 mg/L.
EMERGENCY FINDING: This pediatric patient has classic clinical signs of appendicitis (migratory pain, fever, anorexia) alongside elevated inflammatory markers. This combination demands an urgent targeted ultrasound evaluation.
Ultrasound Findings of Appendicitis
- Non-compressible Appendix: Visualized blind-ended tubular structure measuring greater than 6mm in diameter that fails to collapse under transducer pressure.
- Wall Thickening: Demonstrates a hyperechoic, edematous wall with a characteristic “target sign” cross-section.
- Periappendiceal Fat Changes: Prominent hyperechoic (bright) mesenteric fat surrounding the inflamed appendix.
- Free Fluid: A small volume of complex fluid visualized immediately adjacent to the appendix.
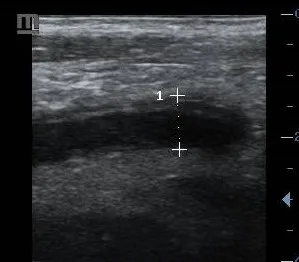
1. Non-compressible appendix: Dilated appendix measuring 8.7mm that completely fails to compress with localized transducer pressure, accompanied by a progressive loss of the normal distinct wall layers.
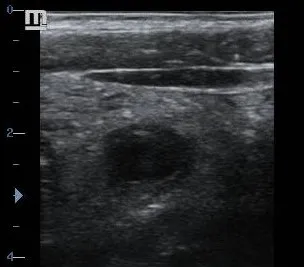
2. Target sign appearance: Concentric rings of alternating hyper- and hypoechogenicity seen in short-axis, indicating marked appendiceal wall edema and acute tissue inflammation.

3. Inflamed periappendiceal fat: Highly echogenic, bright mesenteric fat surrounding the inflamed appendix (marked by asterisk), accompanied by a trace amount of adjacent free pelvic fluid.
Final Diagnosis: Acute Appendicitis
Confirmed key diagnostic features based on the direct correlation of clinical presentation, elevated systemic inflammatory markers, and classical gray-scale ultrasound findings (aperistaltic, non-compressible dilated appendix with surrounding inflammatory fat tracking).
Differential Diagnosis for Right Lower Quadrant Pain
- Mesenteric Adenitis: Characterized by multiple enlarged, hypervascular mesenteric lymph nodes in the RLQ, but demonstrates a completely normal, compressible appendix.
- Omental Infarction: Ultrasound reveals a fixed, focal mass of hyperechoic omental fat that is acutely tender under the probe, with no structural connection to a normal appendix.
- Right Ovarian Pathology (in females): Conditions like ovarian cysts, hemorrhagic cysts, or ovarian torsion present with acute adnexal pain, but present with normal appendiceal structures.
- Diverticulitis (typically in adults): Demonstrates localized colonic wall thickening and outpouchings, leaving the appendix unaffected.
- Gastroenteritis: Presents with diffuse bowel wall thickening and hyperperistalsis (increased bowel activity) often accompanied by clinical diarrhea, with a normal appendix.