Gallbladder Ultrasound
Gallbladder ultrasound is the primary imaging modality for evaluating biliary pathology due to its high sensitivity (91–97%) for gallstones, real-time imaging capabilities, absence of ionizing radiation, and immediate bedside availability.
Anatomy of the gallbladder
- Location: Gallbladder fossa (located on the inferior surface of liver segments IV and V).
- Anatomical Parts:
- Fundus: The rounded, blind end projecting slightly beyond the inferior liver margin.
- Body: The main central segment in direct contact with the liver parenchymal surface.
- Neck: The tapering portion that becomes continuous with the cystic duct (containing the spiral valves of Heister).
- Dimensions: Typically measures 7–10 cm in length and 2.5–4 cm in width.
Clinical indications
1. Basic Indications
- Right upper quadrant (RUQ) abdominal pain
- Suspected cholelithiasis (gallstones)
- Jaundice evaluation
- Abnormal liver function tests (LFTs)
- Fever of unknown origin (to rule out underlying acute cholecystitis)
2. Specific Clinical Scenarios
- Acute cholecystitis: Clinically presenting with localized RUQ pain, fever, and a positive sonographic Murphy’s sign.
- Choledocholithiasis: Biliary obstruction signs including jaundice and elevated alkaline phosphatase (ALP) and gamma-glutamyl transferase (GGT).
- Gallbladder polyps: Incidental finding on abdominal scans, frequently asymptomatic.
Scanning Technique and Preparation
1. Patient Preparation
Ingestion of food, particularly fatty meals, stimulates cholecystokinin release which causes the gallbladder to contract. A contracted gallbladder appears falsely thick-walled and can severely obscure internal luminal or structural wall abnormalities. Consequently, gallbladder evaluations must be performed following a minimum of 4 hours of strict fasting.
Fasting Protocol Limitations:
- < 4 hours: Results in a contracted gallbladder, potentially yielding false-negative findings for small stones or dependent sludge.
- 6–8 hours (Ideal): Achieves maximal physiological distension for optimal lumen and wall visualization.
- > 12 hours: Prolonged fasting can induce stasis, leading to physiologic sludge formation that can mimic active pathology.
2. Equipment Settings
- Transducer: Curvilinear array (3–5 MHz) for routine adult imaging; higher frequency transducers for thin adults or pediatric patients.
- Depth: Adjusted precisely to incorporate the entire gallbladder wall layer and the adjacent porta hepatis anatomy.
- Focal Zones: Set squarely at the level of the gallbladder fossa.
- Harmonic Imaging: Strongly recommended to optimize contrast resolution, reduce reverberation artifacts, and clear out artificial internal echo fill-in.
3. Systematic Scanning Approach
- Subcostal View: Evaluation of the gallbladder in true longitudinal and transverse orthogonal planes.
- Intercostal View: A crucial alternative scanning approach to bypass rib or bowel gas interference, particularly for high-lying gallbladders.
- CBD Evaluation: Tracing the biliary pathway from the gallbladder neck through the porta hepatis down to the pancreatic head.
- Dynamic Maneuvers: Changing patient position (e.g., from supine to left lateral decubitus or standing) is mandatory to demonstrate the mobility of intraluminal contents like stones.
Normal Sonographic Findings
1. Gallbladder
- Pear-shaped, completely anechoic fluid-filled structure.
- Wall thickness measures strictly < 3 mm.
- Demonstrates clear acoustic enhancement posteriorly with no internal echoes (except occasionally dependent, mobile physiologic sludge).
- Normal length ranges between 7–10 cm, with width measuring < 4 cm.
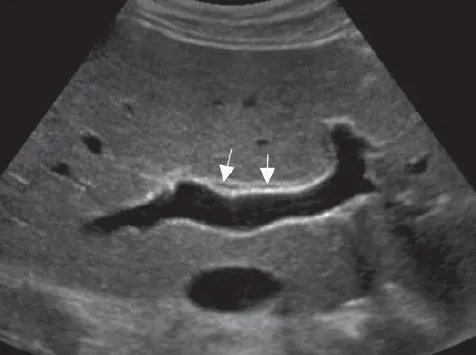
2. Bile Ducts
- Normal ductal walls appear as thin, regular echogenic lines bounding an anechoic lumen.
- Absence of intraluminal masses, strictures, or impacted calculi.
- No periductal edema or pathologically increased color Doppler vascularity.
:::tip[Landmark: Portal Triad] The “Mickey Mouse” sign represents the anatomy of the portal triad visualized in cross-section:
- Head: Portal vein (the largest, posterior structure)
- Left ear: Common bile duct (located anteriorly and laterally)
- Right ear: Hepatic artery (the smallest structure, located anteriorly and medially) :::

Pathological Findings
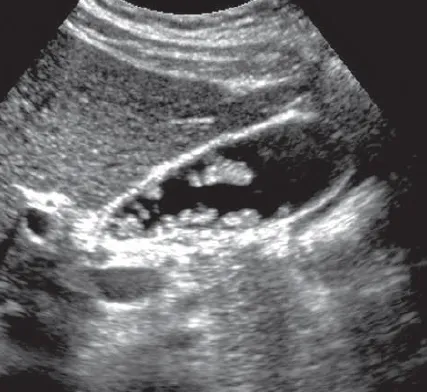
1. Cholelithiasis (Gallstones)
- Findings: Highly reflective, mobile hyperechoic intraluminal focus demonstrating discrete posterior acoustic shadowing.
- WES Triad (Wall-Echo-Shadow): Visualized in a shrunken, contracted gallbladder fully packed with stones. The sonographer identifies the echogenic gallbladder wall, the echogenic stone surface immediately deep to it, followed by a dense acoustic shadow.
- Complications: Can progress to acute cholecystitis, gallbladder empyema, or mural calcification (porcelain gallbladder).
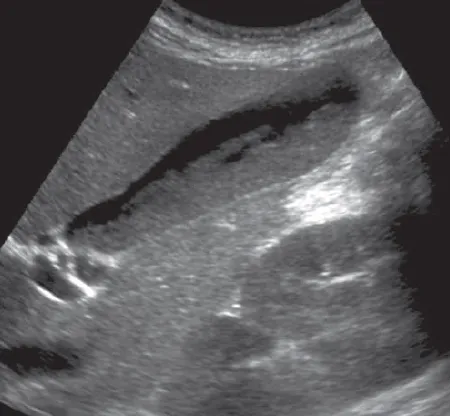
2. Biliary Sludge
A particulate suspension consisting of calcium bilirubinate granules and cholesterol crystals precipitating out of stagnant bile. It presents as amorphous, low-level internal echoes layering in the dependent portion of the gallbladder lumen. It forms a straight horizontal fluid-fluid level, moves slowly with positional changes, and lacks posterior acoustic shadowing.
3. Acute Cholecystitis
Characterized by gallbladder wall thickening (> 3 mm), transient distension, pericystic fluid collections, and impacted stones in the gallbladder neck triggering a positive sonographic Murphy’s sign.
- Gangrenous Cholecystitis: Indicated by an asymmetric, irregular wall with focal sloughing of intraluminal membranes, internal hemorrhage/debris bands, and microabscesses within the wall layers.
- Perforated Gallbladder: Identified by a focal defect or visible rent in the gallbladder wall. Secondary signs include a localized pericholecystic fluid collection/abscess and a rapid loss of the typical distended, gourdlike gallbladder shape.
- Emphysematous Cholecystitis: A surgical emergency triggered by gas-producing organisms (often following ischemic events). It manifests as bright echogenic lines within the wall or lumen displaying “dirty” acoustic shadowing, ring-down, or reverberation artifacts.
- Acalculous Cholecystitis: Acute inflammation presenting with wall thickening and pericholecystic fluid but without shadowing gallstones; frequently encountered in critically ill or severely traumatized patients.
4. Torsion (Volvulus) of the Gallbladder
A rare condition characterized by a massively distended, inflamed gallbladder oriented horizontally along a left-to-right axis. A definitive structural twist of the cystic duct and cystic artery may be directly visualized. Torsion exceeding 180 degrees rapidly induces hemorrhagic gangrene, requiring emergency surgery.
5. Chronic Cholecystitis
Almost invariably associated with recurrent irritation from gallstones. Sonographically demonstrates a variable degree of gallbladder wall fibrosis or thickening alongside persistent calculi, though patients are frequently asymptomatic between mild clinical episodes.
6. Porcelain Gallbladder
Extensive mural calcification of the gallbladder wall secondary to chronic inflammation. The sonographic appearance depends on the pattern of calcification:
- Dense, continuous calcification: Presents as a smooth, hyperechoic semilunar line showing dense, clean posterior acoustic shadowing, which completely obscures the lumen. This can mimic a large gallstone but lacks a clear wall superficial to the echo.
- Mild, patchy calcification: Displays an irregular echogenic mural border with variable posterior shadowing, allowing partial evaluation of internal luminal contents.
7. Adenomyomatosis (Adenomatous Hyperplasia)
A benign hyperplastic condition characterized by overgrowth of the mucosa and thickening of the muscular layer, leading to invaginations known as Rokitansky-Aschoff sinuses. Its hallmark sonographic appearance features small, intramural echogenic foci that generate prominent V-shaped comet-tail (reverberation) artifacts, caused by cholesterol crystals trapped within these tiny cystic spaces.
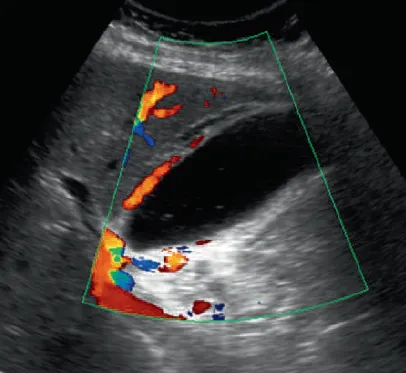
8. Polypoid Masses of the Gallbladder
- Cholesterol Polyps: The most common gallbladder polyps; present as multiple, small (< 10 mm), ovoid, highly echogenic fixed masses attached to the wall that do not shadow and do not move with changes in patient position.
- Adenomas and Inflammatory Polyps: True benign neoplasms, typically pedunculated and single. Larger adenomatous lesions (> 10 mm) show internal vascularity on power Doppler and carry a heightened risk of focal malignant transformation. They present with a more heterogeneous echotexture as they grow.
9. Malignancies
Primary gallbladder carcinoma typically manifests as a large, heterogeneous soft-tissue mass replacing or distorting the gallbladder fossa, an asymmetric or focal mural thickening, or a polypoid mass expanding into the lumen. It is frequently accompanied by disrupted wall layers, local liver invasion, and regional lymphadenopathy.





References
- American College of Radiology (ACR). (2023). ACR Appropriateness Criteria® Right Upper Quadrant Pain. Journal of the American College of Radiology, 20(1S), S12-S24.
- Middleton, W. D., et al. (2022). Ultrasound: The Requisites (4th ed.). Elsevier.
- Rumack, C. M., & Levine, D. (2021). Diagnostic Ultrasound (6th ed.). Elsevier.
- National Institute for Health and Care Excellence (NICE). (2022). Gallstone disease: diagnosis and management. NICE Clinical Guideline 188.
- European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB). (2021). Guidelines on Interventional Ultrasound. Ultraschall in der Medizin, 42(1), 12-45.