Biliary Tree Ultrasound
Ultrasound is the primary imaging modality for evaluating the biliary system due to its non-invasive nature, absence of ionizing radiation, real-time imaging capabilities, and widespread availability. It serves as the initial investigation for suspected biliary pathology with a sensitivity of 91–97% for detecting gallstones.
Anatomy of the biliary tree
The biliary system consists of a series of ducts that transport bile from the liver to the duodenum:
- Intrahepatic bile ducts: Follow portal triads (parallel to portal veins)
- Right and left hepatic ducts: Merge to form the common hepatic duct (CHD)
- Cystic duct: Connects gallbladder to CHD
- Common bile duct (CBD): Formed by union of CHD and cystic duct
Indications for Biliary Ultrasound
1. Common Clinical Scenarios
- Right upper quadrant (RUQ) abdominal pain
- Suspected cholelithiasis or choledocholithiasis
- Jaundice (obstructive vs. hepatocellular)
- Abnormal liver function tests (especially elevated ALP and GGT)
- Fever of unknown origin (screening for cholangitis)
2. Specific Clinical Indications
- Acute cholecystitis: RUQ pain + fever + leukocytosis
- Biliary obstruction: Jaundice + pruritus + pale stools
- Post-liver transplant: Monitor for biliary strictures
- Chronic liver disease: Evaluate for secondary biliary changes
Scanning Technique and Preparation
1. Patient Preparation
- Fasting: 6–8 hours (reduces bowel gas and gallbladder contraction)
- Positioning: Supine or left lateral decubitus (improves CBD visualization)
- Breathing instructions: Instruct patient to hold breath in expiration
2. Equipment Settings
- Transducer: Curvilinear (3–5 MHz) for adults, higher frequency for pediatrics
- Depth: Adjust to include entire biliary tree (typically 12–16 cm)
- Harmonic imaging: Reduces artifacts and improves resolution
- Focal zones: Set at level of porta hepatis
3. Systematic Scanning Approach
- Subcostal view: Identify gallbladder and portal triad
- Intercostal view: Assess intrahepatic ducts
- CBD tracing: Follow from porta hepatis to pancreatic head
- Color Doppler: Differentiate ducts from vessels
Normal Sonographic Findings
1. Gallbladder
- Pear-shaped anechoic structure
- Wall thickness < 3 mm
- No internal echoes (except dependent sludge)
- Normal length 7–10 cm, width < 4 cm
2. Bile Ducts
- Walls appear as thin echogenic lines
- Lumen is anechoic
- No intraductal masses or calculi
- No periductal edema or vascularity
:::tip[Landmark: Portal Triad] The “Mickey Mouse” sign represents the portal triad in cross-section:
- Head: Portal vein (largest)
- Left ear: Common bile duct
- Right ear: Hepatic artery (smallest) :::

Pathological Findings
1. Cholelithiasis (Gallstones)
- Findings: Mobile hyperechoic focus with posterior acoustic shadowing.
- WES triad: Wall-Echo-Shadow complex characteristic of a contracted gallbladder packed with stones.
- Complications: Cholecystitis, empyema, porcelain gallbladder.
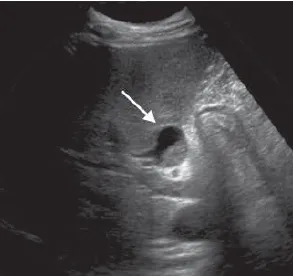
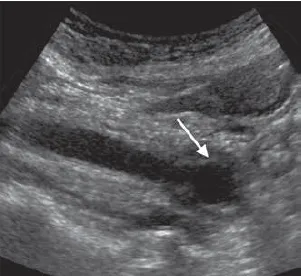
2. Choledocholithiasis (CBD Stones)
- Findings: Echogenic intraluminal focus within the bile duct with posterior shadowing.
- Dilation: CBD > 6 mm with associated proximal ductal dilation.
- Twinkling artifact: May be visible on color Doppler behind small or tightly wedged calculi.
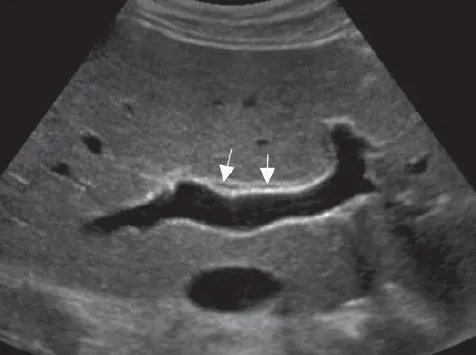
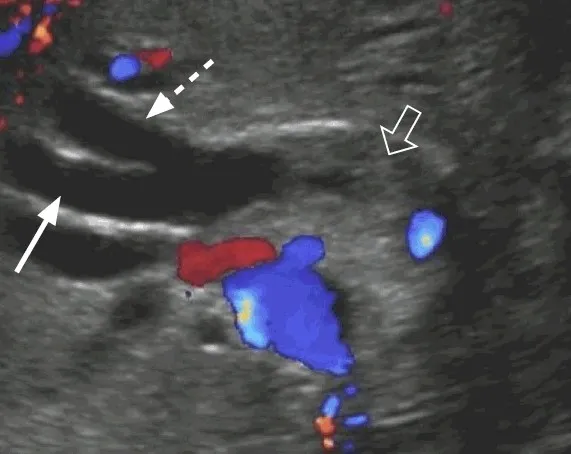
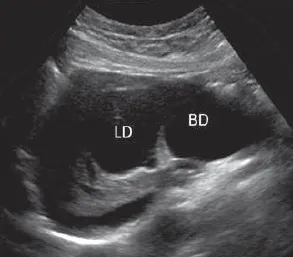
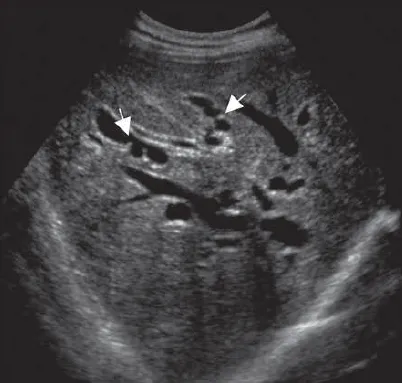
3. Biliary Obstruction
- Intrahepatic: “Too many tubes” sign or “shotgun” sign indicating multiple dilated intrahepatic bile ducts running parallel to portal branches.
- Extrahepatic: “Double barrel” sign representing a simultaneously dilated CBD and portal vein.
- Causes: Stones (75%), tumors (20%), strictures (5%).
4. Cholangitis
- Findings: Ductal dilation accompanied by diffuse ductal wall thickening and intraluminal echogenic debris (pus/sludge).
- Clinical Correlation: Often presents with Charcot’s triad (fever, jaundice, RUQ pain).
5. Choledochal Cysts
- Type I: Fusiform dilation of the CBD, representing the most common variant (80%).
- Type II: True diverticula arising from the bile ducts (very rare).
- Type III: Choledochoceles, which are confined to the intraduodenal portion of the CBD.
- Type IV: - Type IVa: Multiple intrahepatic and extrahepatic biliary dilations.
- Type IVb: Dilations confined strictly to the extrahepatic biliary tree.
- Type V: Caroli disease has historically been classified here, though it carries a distinct embryonic origin.
6. Caroli Disease
A rare congenital disorder characterized by segmental, non-obstructive saccular or fusiform dilation of the intrahepatic bile ducts. It leads to biliary stasis, stone formation, and recurrent bouts of cholangitis and sepsis. Unlike recurrent pyogenic cholangitis, the ductal contents do not form a rigid structural cast of the system.
7. Mirizzi Syndrome
A rare complication of chronic gallstone disease where an impacted gallstone in the cystic duct or gallbladder neck causes extrinsic compression and obstruction of the adjacent common hepatic duct (CHD).
- Dilated CHD and intrahepatic ducts above the level of obstruction with a normal CBD below.
- Impacted stone visualized as a hyperechoic focus with shadowing in the gallbladder neck.
- Biliary-enteric “parallel channel” sign may be present along the portal vein.
8. Hemobilia
Often secondary to iatrogenic biliary trauma (percutaneous procedures, liver biopsies), vascular malformations, or abdominal trauma. Acute hemorrhage appears as low-level fluid echoes, whereas older blood clots appear as echogenic, mixed-echogenicity, or retractile masses conforming to the duct shape.
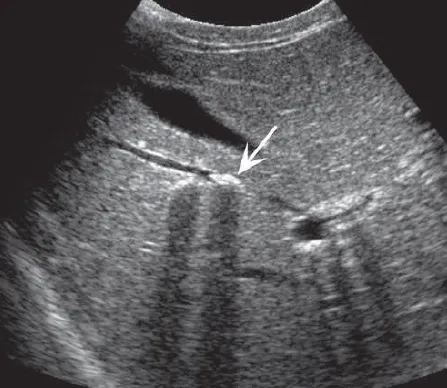
9. Pneumobilia
Refers to air within the biliary tree, commonly seen post-sphincterotomy, post-ERCP, or secondary to a biliary-enteric fistula. Appears as bright, echogenic linear structures following the portal triads, typically in a nondependent position, associated with “dirty” acoustic shadowing, reverberation, and ring-down artifacts.
10. Biliary Tree Infections
Includes acute bacterial ascending cholangitis, liver flukes, recurrent pyogenic cholangitis, ascariasis, and HIV cholangiopathy.
11. Immune-Related Diseases
Conditions causing specific biliary changes include Primary Biliary Cholangitis (PBC), Primary Sclerosing Cholangitis (PSC), and IgG4-related cholangitis.
12. Malignancies (Cholangiocarcinoma & Metastases)
- Cholangiocarcinoma: Can manifest as intrahepatic masses or hilar tumors (Klatskin tumors) causing abrupt segment-specific ductal obstruction.
- Metastases: Biliary tree metastases can closely mimic cholangiocarcinoma. Common primary sites include the breast, colon, and melanoma.
:::danger[Critical Findings Requiring Urgent Intervention]
- CBD stone with clinical signs of ascending cholangitis (requires emergency ERCP)
- Gallbladder empyema or gangrenous cholecystitis (high risk of perforation)
- Biliary-enteric fistula associated with bowel obstruction (gallstone ileus) :::






Conclusion
Ultrasound remains the first-line imaging modality for biliary tree evaluation, offering excellent diagnostic accuracy for common conditions like cholelithiasis and biliary obstruction while avoiding radiation exposure. Proper technique—including patient preparation, correct transducer selection, and a systematic scanning approach—is essential for optimal results.
While ultrasound has structural limitations in evaluating the distal CBD due to overlying bowel gas, it provides crucial initial diagnostic information that directly guides further clinical management, such as the need for advanced MRCP imaging or therapeutic ERCP interventions.
References
- American College of Radiology (ACR). (2022). ACR Appropriateness Criteria® Right Upper Quadrant Pain. Journal of the American College of Radiology, 19(5S), S223-S231.
- Middleton, W. D., Kurtz, A. B., & Hertzberg, B. S. (2021). Ultrasound: The Requisites (4th ed.). Elsevier.
- Rumack, C. M., Levine, D. (2022). Diagnostic Ultrasound (6th ed.). Elsevier.
- European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB). (2020). Guidelines on Interventional Ultrasound (INVUS), Part III - Abdominal Treatment Procedures. Ultraschall in der Medizin, 41(1), 16-44.
- National Institute for Health and Care Excellence (NICE). (2021). Gallstone disease: diagnosis and management. NICE Clinical Guideline 188.