Biliary Tree Infections
Biliary tract infections encompass a wide spectrum of conditions ranging from acute bacterial infections to chronic parasitic infestations. Ultrasound serves as the primary imaging modality due to its excellent soft tissue differentiation, real-time imaging capability, and lack of ionizing radiation. This article details the sonographic appearance of five clinically significant biliary infections:
- Ascending cholangitis - Bacterial infection of obstructed bile ducts
- Liver fluke infections - Parasitic infestations (Clonorchis, Opisthorchis, Fasciola)
- Recurrent pyogenic cholangitis - Oriental cholangiohepatitis
- Biliary ascariasis - Worm infestation of biliary tree
- HIV cholangiopathy - AIDS-related biliary disease
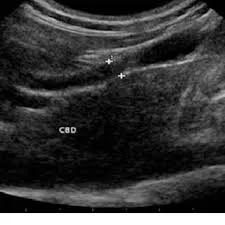
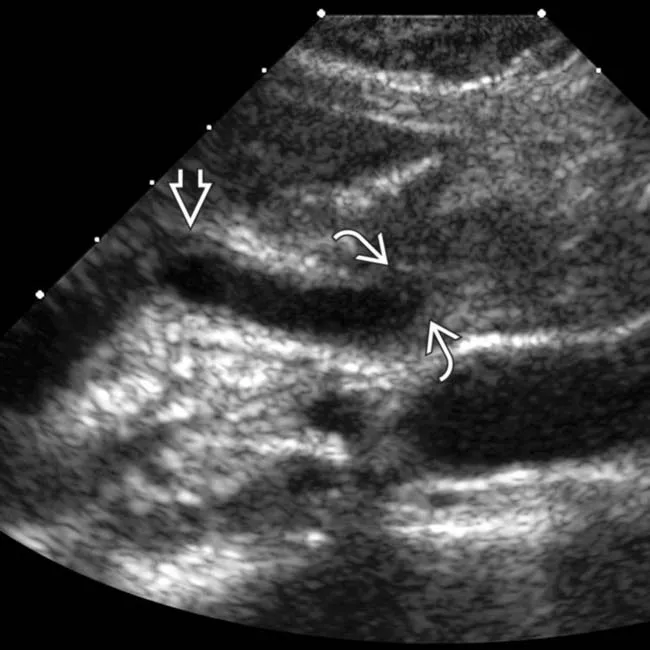
1. Ascending cholangitis
Acute bacterial infection secondary to biliary obstruction, most commonly from stones (70%), followed by strictures and tumors.
Pathophysiology
Obstruction → bacterial overgrowth (E. coli, Klebsiella, Enterococcus) → increased ductal pressure → systemic infection.
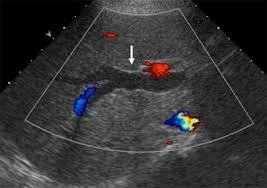
Ultrasound Findings
- Bile duct dilation (CBD > 8mm, intrahepatic > 2mm)
- Echogenic debris within ducts (pus/sludge)
- Pneumobilia (20% of cases) - bright echoes with “dirty” shadowing
- Gallstones or other obstructive lesions
- Portal vein thrombosis in severe cases


2. Liver Fluke Infections
Chronic parasitic infestations caused by Clonorchis sinensis, Opisthorchis viverrini (Asian liver flukes), and Fasciola hepatica (sheep liver fluke).
Epidemiology & Life Cycle
Endemic in Southeast Asia. Humans ingest metacercariae in raw fish (Clonorchis) or water plants (Fasciola) → larvae migrate to bile ducts → mature into adult flukes.
Ultrasound Findings
- Ductal wall thickening (fibrosis from chronic irritation)
- Intrahepatic duct dilation with normal CBD (60% of cases)
- Fluke visualization (2–10mm echogenic foci in ducts)
- Periductal fibrosis (hyperechoic streaks)
- Gallbladder sludge/stones (common complication)

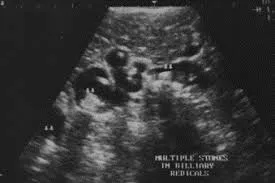
3. Recurrent Pyogenic Cholangitis (RPC)
Also called Oriental cholangiohepatitis, common in Southeast Asia. Characterized by recurrent bacterial cholangitis with intrahepatic pigment stones.
Pathogenesis
Chronic parasitic infection (flukes/ascaris) → bile stasis → bacterial colonization → stone formation → recurrent infection cycles.
Ultrasound Findings
- Segmental intrahepatic duct dilation (left lobe predominance)
- Intraductal stones (cast-like, non-shadowing)
- Ductal strictures with abrupt caliber changes
- Parenchymal atrophy of affected segments
- Portal vein thrombosis in advanced cases
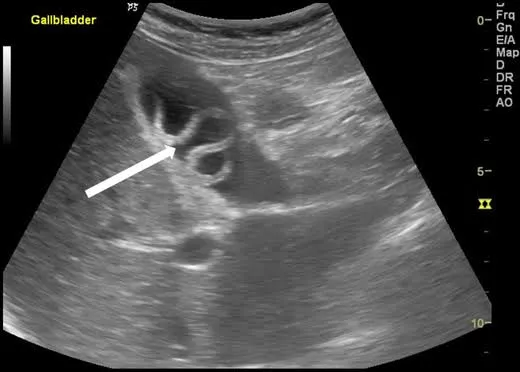
4. Biliary Ascariasis
Infestation by Ascaris lumbricoides, the largest intestinal nematode (15–35cm long).
Ultrasound Findings
- Long tubular structure in bile ducts (4–6mm diameter)
- Parallel echogenic lines (worm’s digestive tract)
- Spaghetti sign - coiled worms in gallbladder
- Real-time movement of worms (diagnostic)
- Ductal dilation proximal to obstruction
Clinical Management
Albendazole/mebendazole therapy. ERCP for extraction if worms don’t retreat to intestine within 3 days.

5. HIV Cholangiopathy
AIDS-related biliary disease occurring when CD4 counts < 100 cells/mm³, caused by opportunistic infections (Cryptosporidium, CMV, Microsporidia).
Ultrasound Findings
- Ductal wall thickening (>1.5mm)
- Strictures (focal or diffuse)
- Papillary stenosis (CBD dilation > 12mm)
- Intrahepatic duct irregularity (beaded appearance)
- Gallbladder wall thickening (acalculous cholecystitis)
Treatment Approach
Antiretroviral therapy (ART) is primary treatment. ERCP with sphincterotomy for symptomatic relief.

Comparative Ultrasound Features
| Condition | Key Ultrasound Feature | Pathognomonic Sign |
|---|---|---|
| Ascending cholangitis | Dilated ducts + echogenic debris | Pneumobilia |
| Liver flukes | Ductal wall thickening | Visible flukes in ducts |
| RPC | Left lobe ductal dilation | Cast-like intraductal stones |
| Ascariasis | Long tubular structure | Parallel echogenic lines |
| HIV cholangiopathy | Ductal wall thickening | Beaded intrahepatic ducts |
References
- Lim JH. Liver flukes: the malady neglected. Korean J Radiol. 2011;12(3):269-279. doi:10.3348/kjr.2011.12.3.269
- Kiriyama S, Kozaka K, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholangitis. J Hepatobiliary Pancreat Sci. 2018;25(1):17-30. doi:10.1002/jhbp.512
- Chan HH, Lai KH, Lin CK, et al. Endoscopic diagnosis and management of biliary parasitosis. Diagn Ther Endosc. 2011;2011:376023. doi:10.1155/2011/376023
- Lim JH, Kim SY, Park CM. Parasitic diseases of the biliary tract. AJR Am J Roentgenol. 2007;188(6):1596-1603. doi:10.2214/AJR.06.1172
- Catalano OA, Sahani DV, Forcione DG, et al. Biliary infections: spectrum of imaging findings and management. Radiographics. 2009;29(7):2059-2080. doi:10.1148/rg.297095051
- Raman SP, Horton KM, Fishman EK. Multimodality imaging of pancreatic and biliary neoplasms. Surg Oncol Clin N Am. 2014;23(4):649-689. doi:10.1016/j.soc.2014.06.002
- Baron TH, Davee T. AIDS cholangiopathy. Curr Treat Options Gastroenterol. 2003;6(2):111-117. doi:10.1007/s11938-003-0002-0
- Park MS, Yu JS, Kim KW, et al. Recurrent pyogenic cholangitis: comparison between MR cholangiography and direct cholangiography. Radiology. 2001;220(3):677-682. doi:10.1148/radiol.2203001424
- Rumack CM, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier; 2018.
- American Institute of Ultrasound in Medicine (AIUM). AIUM practice guideline for the performance of ultrasound examinations of the abdomen and/or retroperitoneum. J Ultrasound Med. 2021;40(7):E1-E16. doi:10.1002/jum.15607